


Childbirth as a Spectator Sport
Good Time Girls
When Agnodice Became a Handbag…
Love, Sex, and Cuddly Cupids
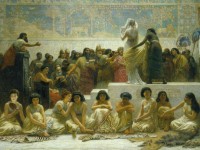
Bed, Bread and Dead: The Dummies’ Guide to Herodotus

Agnodice: Down and Dirty?

The history of tampons – in ancient Greece?

The Blue Books: Guides to the New Orleans Red Light District
- « Previous Page
- 1
- 2
- 3
- 4
- …
- 8
- Next Page »